

The Agitated Behavior Scale (ABS) is a 14-item observational rating tool developed by John D. Corrigan, Ph.D., at Ohio State University in 1989 to measure agitation severity during the acute recovery phase following traumatic brain injury (TBI), particularly during posttraumatic amnesia (PTA). Each item is rated on a 1–4 scale (1 = absent, 4 = extreme), yielding a total score range of 14 to 56. A score of 21 or below is considered normal; scores of 22–28 indicate mild agitation, 29–35 moderate, and 36–56 severe agitation (Corrigan, 1989). The ABS demonstrates strong internal consistency (Cronbach's alpha 0.83–0.92) and excellent inter-rater reliability for total scores (r = 0.92). Zentake's digital ABS enables bedside staff to complete observations efficiently with automatic scoring and longitudinal tracking.
Raters observe the patient for a defined observation period (typically 30 minutes to 8 hours) and rate each of the 14 behaviors on a scale from 1 to 4. Ratings are summed to produce a total score ranging from 14 to 56. Severity interpretation is as follows:
Three subscales have also been identified: Aggression (physical and verbal assault), Disinhibition (impulsive and socially inappropriate behavior), and Lability (emotional instability). Zentake automatically calculates the ABS total score and subscale scores upon each observation entry, enabling real-time clinical decision support.
Step 1: Identify the observation period. Clinicians or trained rehabilitation staff select a structured observation window, typically an 8-hour nursing shift or a designated 30-minute observation block. Zentake allows staff to set observation periods digitally and receive reminders.
Step 2: Observe the patient directly. The rater watches the patient during normal care activities — not through interview or retrospective report. All 14 ABS behaviors should be observed during natural interactions such as repositioning, meals, or therapy sessions.
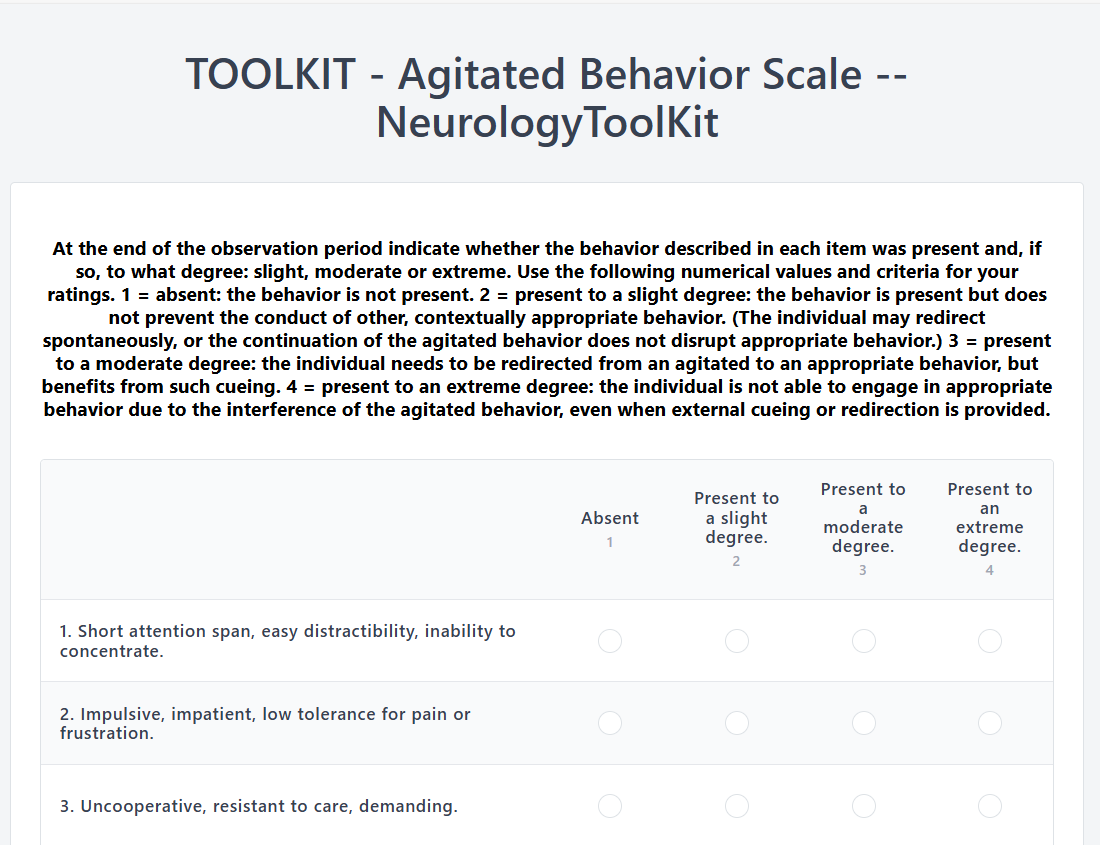
Step 3: Rate each behavior on the 1–4 scale. For each item, score 1 (absent), 2 (present to a slight degree), 3 (present to a moderate degree), or 4 (present to an extreme degree). Do not base ratings on a single incident; consider the full observation period.
Step 4: Calculate the total and subscale scores. Sum all 14 item scores to get the total ABS score. With Zentake, scoring is automatic upon submission — no manual addition required.
Step 5: Document and track longitudinally. Record the score alongside clinical notes. Zentake stores all ABS scores over time, enabling your team to visualize agitation trajectories and evaluate intervention efficacy across the patient's inpatient stay.
Scoring: Paper ABS requires manual addition of 14 items per observation. Zentake calculates total and subscale scores instantly upon submission, eliminating arithmetic errors.
Completion: Paper forms can be misplaced during busy shifts. Zentake's mobile-friendly interface allows bedside staff to submit observations from any device in under 2 minutes.
Delivery: Paper forms must be retrieved, copied, and filed. Zentake delivers the ABS digitally to any clinician on the care team, accessible in real time.
Data Storage: Paper records risk loss, illegibility, and physical damage. Zentake stores all ABS data securely in the cloud under HIPAA-compliant encryption.
Longitudinal Tracking: Paper records require manual comparison across shifts. Zentake automatically generates agitation trajectory graphs, making it easy to see whether a patient is improving, stable, or deteriorating.
Security: Paper offers no audit trail. Zentake logs every submission with timestamps and user identifiers, supporting compliance and chain-of-care documentation.
Integration: Paper data must be manually transcribed into the EHR. Zentake integrates with EMR platforms to push ABS scores directly into the patient record.
Cost: Paper forms incur printing, filing, and labor overhead. Zentake replaces these costs with a scalable digital platform that grows with your program.
What does the Agitated Behavior Scale measure?
The ABS measures agitation and problematic behaviors that occur during the acute recovery phase following traumatic brain injury, specifically during posttraumatic amnesia. It assesses 14 behaviors including restlessness, distractibility, impulsivity, aggression, and emotional lability — rated on a 1–4 scale during a structured observation period. Zentake digitalizes this observation process so clinicians can submit ratings directly from the bedside.
How do you score the ABS?
Each of the 14 items is rated 1 (absent) to 4 (extreme), and scores are summed to produce a total ranging from 14 to 56. Scores ≤21 are normal, 22–28 mild, 29–35 moderate, and 36–56 severe agitation. Zentake automatically calculates these scores upon submission, eliminating manual computation.
Who developed the Agitated Behavior Scale?
The ABS was developed by John D. Corrigan, Ph.D., and colleagues at Ohio State University, first published in 1989. It was developed specifically to fill a gap in objective measurement tools for agitation during the posttraumatic amnesia phase of TBI recovery.
Who administers the ABS?
The ABS is completed by direct-care staff who observe the patient — typically nursing staff, rehabilitation therapists, or trained rehabilitation technicians. It is not a patient self-report tool; it requires trained observation during actual patient care activities.
How long does ABS administration take?
The observation period typically spans a nursing shift (8 hours) or a dedicated 30-minute observation window. Completing the rating form itself takes approximately 5 minutes after the observation period. Zentake's digital form is optimized for quick bedside entry on any device.
What population is the ABS designed for?
The ABS is designed for individuals with acquired brain injury — primarily traumatic brain injury — who are in the acute recovery phase and experiencing posttraumatic amnesia. It has been validated in patients ranging from age 16 to 92, and adapted versions have been studied in pediatric TBI populations.
Is the ABS free to use?
The ABS instrument itself is publicly available and widely used without licensing fees. Zentake provides the digital ABS platform with HIPAA-compliant data storage, automated scoring, and EMR integration as part of its subscription plans. Start your free trial at zentake.com.
What are the ABS subscales?
The ABS contains three empirically derived subscales: Aggression (items related to striking, biting, or screaming), Disinhibition (impulsive, socially inappropriate behavior), and Lability (rapid emotional shifts). These subscales can help guide targeted interventions for different aspects of agitated behavior.
1. Corrigan, J. D. (1989). Development of a scale for assessment of agitation following traumatic brain injury. Journal of Clinical and Experimental Neuropsychology, 11(2), 261–277. https://doi.org/10.1080/01688638908400888
2. Bogner, J. A., Corrigan, J. D., Fugate, L., Mysiw, W. J., & Clinchot, D. (2001). Rating scale analysis of the Agitated Behavior Scale. Journal of Head Trauma Rehabilitation, 16(2), 144–154. https://doi.org/10.1097/00001199-200104000-00004
3. Nott, M. T., Chapparo, C., & Baguley, I. J. (2006). Agitation following traumatic brain injury: an Australian sample. Brain Injury, 20(11), 1175–1182. https://doi.org/10.1080/02699050601049114
Last updated: April 2026
The leading patient intake platform. HIPAA compliant forms for healthcare providers and organizations. Find out what you're missing!



