

The Katz Index of Independence in Activities of Daily Living (Katz ADL) is a validated six-item geriatric assessment that measures a patient's ability to perform basic self-care activities independently — bathing, dressing, toileting, transferring, continence, and feeding. Developed by Sidney Katz and colleagues in 1963, it remains one of the most widely used functional-status instruments in primary care, hospital, rehabilitation, skilled nursing, and home health settings. Zentake's HIPAA-compliant digital platform lets clinicians administer the Katz ADL, auto-score results, trend functional change over time, and route documentation directly into the EHR.
The Katz ADL takes only a few minutes to complete and produces a clear 0–6 score that quantifies functional independence at a single point in time. Because the items map to concrete self-care tasks, clinicians can administer it consistently across nursing staff, therapists, and physicians without specialized training, making it ideal for high-volume admission workflows.
Serial Katz ADL scores let care teams quantify functional decline in chronic-disease populations and document measurable recovery in post-acute or rehabilitation settings. Repeated administration is the standard way to detect a new functional deficit that warrants further geriatric, neurologic, or physical-therapy workup.
Functional status is a strong predictor of hospitalization, falls, institutionalization, and 30-day readmission. Katz ADL scores inform discharge planning, level-of-care decisions for skilled nursing and home health referrals, and the design of personalized care plans for medically complex older adults.
Functional assessments are required components of comprehensive geriatric evaluation, Medicare Annual Wellness Visits, OASIS home health documentation, and many value-based-care quality programs. A standardized score in the chart supports billing, audit defense, and population-health reporting.
Primary Care & Geriatrics: Used at annual wellness visits and chronic-care visits to flag emerging functional decline that may signal cognitive impairment, frailty, or medication-related harm.
Hospital & Inpatient Medicine: Administered on admission to establish a functional baseline, then re-administered before discharge to guide post-acute placement decisions.
Skilled Nursing & Long-Term Care: Used at admission, quarterly, and on significant change of condition to support care-plan revision and MDS documentation.
Home Health & Rehabilitation: Tracks recovery after stroke, hip fracture, or hospitalization and helps therapists set measurable functional goals.
Telehealth & Remote Monitoring: Caregivers or patients can complete the Katz ADL from home before a virtual visit, giving the clinician a structured functional snapshot to anchor the encounter.
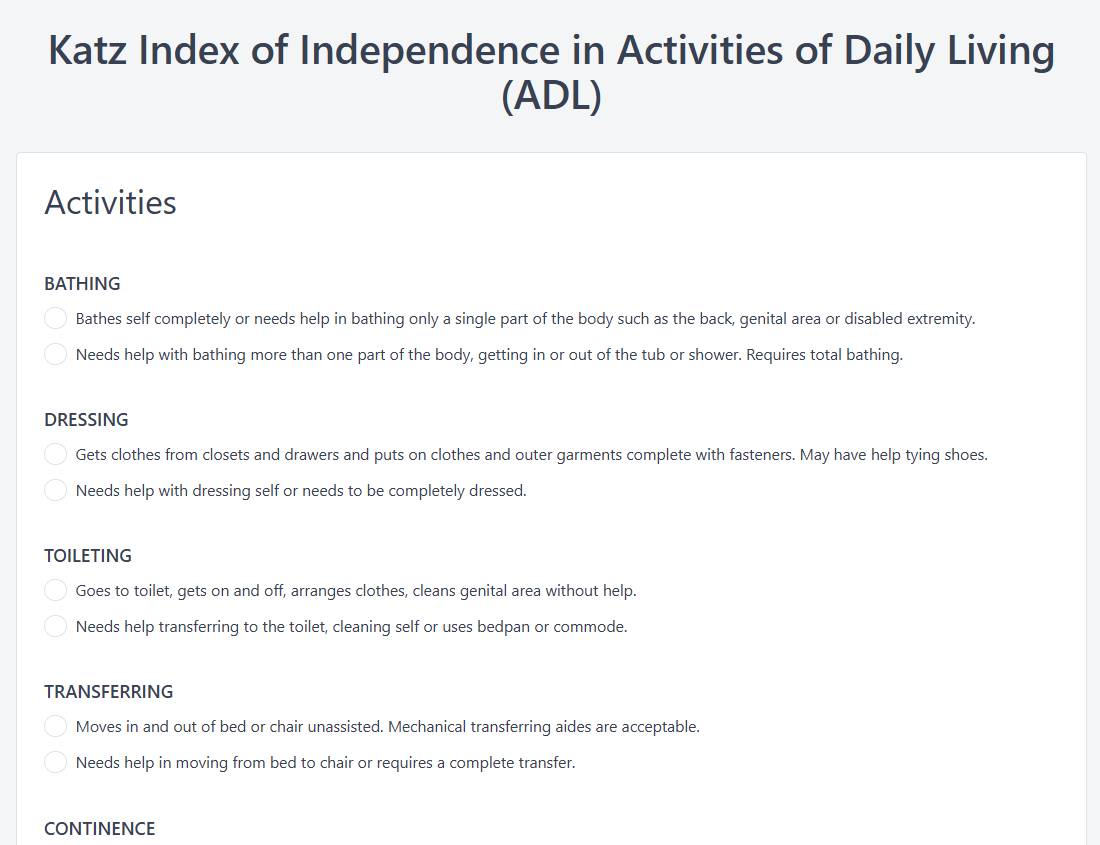
Each activity is rated as independent (1 point) or dependent (0 points). The six domains are:
Scores are summed across the six items for a total ranging from 0 to 6.
| Score | Interpretation | Typical Clinical Implication |
|---|---|---|
| 6 | Full function | Independent in all ADLs; routine monitoring |
| 4 | Moderate impairment | Targeted support and reassessment of contributing factors |
| 2 or less | Severe functional impairment | Comprehensive evaluation and higher level of care planning |
| 0 | Very dependent | Dependent in all six activities; intensive caregiver or facility support |
The Katz ADL has demonstrated strong internal consistency, interrater reliability, and test–retest reliability across diverse geriatric populations and multiple language validations.
Functional status documentation supports Medicare Annual Wellness Visit requirements, OASIS-E reporting in home health, MDS documentation in skilled nursing facilities, and quality measures tied to fall risk, dementia care, and care-transition programs. Storing scores in a structured, auditable record helps organizations defend reimbursement and respond to chart audits.
Any trained clinical team member can administer the Katz ADL — physicians, advanced-practice clinicians, registered nurses, physical and occupational therapists, social workers, and home-health aides under clinical supervision. Because the scoring is binary and the items map to observable behaviors, the tool produces consistent results across roles when administered with standard instructions.
Most patients or informants complete the Katz ADL in two to five minutes. With Zentake's automated scoring, the total and per-item results are available immediately on submission, so the assessment fits easily into intake workflows, annual wellness visits, and admission documentation without extending visit time.
Yes. The Katz ADL has been used and validated since 1963 across hospitalized, community-dwelling, long-term-care, and rehabilitation populations, and has been translated and validated in multiple languages. Studies consistently report strong internal consistency, interrater reliability, and predictive validity for outcomes including hospitalization, institutionalization, and mortality.
The Katz ADL measures basic self-care activities (bathing, dressing, toileting, transferring, continence, feeding). The Lawton Instrumental ADL Scale measures more complex activities required to live independently in the community (managing money, medications, transportation, telephone, shopping, food preparation, housekeeping, laundry). Many geriatric assessments use both together for a complete functional picture.
Yes. Zentake's measures feature stores each Katz ADL administration against the patient record so clinicians can view scores chronologically, see directional change at a glance, and use trend data to support care-plan revisions, discharge decisions, and quality reporting.
No. The Katz ADL is one component of a comprehensive geriatric assessment. It is best paired with cognitive screening, mood assessment, gait and balance evaluation, medication reconciliation, and a review of social supports. The Katz score informs but does not replace clinical judgment about diagnosis or level of care.
Last updated: May 2026.
The leading patient intake platform. HIPAA compliant forms for healthcare providers and organizations. Find out what you're missing!



