

The ABCD2 and ABCD3-I scores are clinical prediction tools used to estimate the short-term risk of stroke following a transient ischemic attack (TIA). The ABCD2 score was developed by Johnston, Rothwell, and colleagues in 2007 and uses five clinical parameters — age, blood pressure, clinical features, symptom duration, and diabetes status — to produce a score ranging from 0 to 7 (Johnston et al., Lancet, 2007). The ABCD3-I score, proposed by Merwick et al. in 2010, extends this to a 13-point scale by adding dual TIA events and neuroimaging findings (Lancet Neurology, 2010). Both tools demonstrate strong sensitivity for identifying patients at elevated stroke risk within 2, 7, and 90 days after a TIA. Zentake's digital version allows clinicians to administer and auto-score both tools in a HIPAA-compliant environment.
The ABCD2 score is calculated by summing points from five clinical parameters. The total score ranges from 0 to 7. Risk categories based on the ABCD2 are: low risk (0–3 points, approximately 1% 2-day stroke risk), moderate risk (4–5 points, approximately 4% 2-day stroke risk), and high risk (6–7 points, approximately 8% 2-day stroke risk). A score of 4 or higher warrants urgent specialist evaluation and potential hospitalization (Johnston et al., Lancet, 2007).
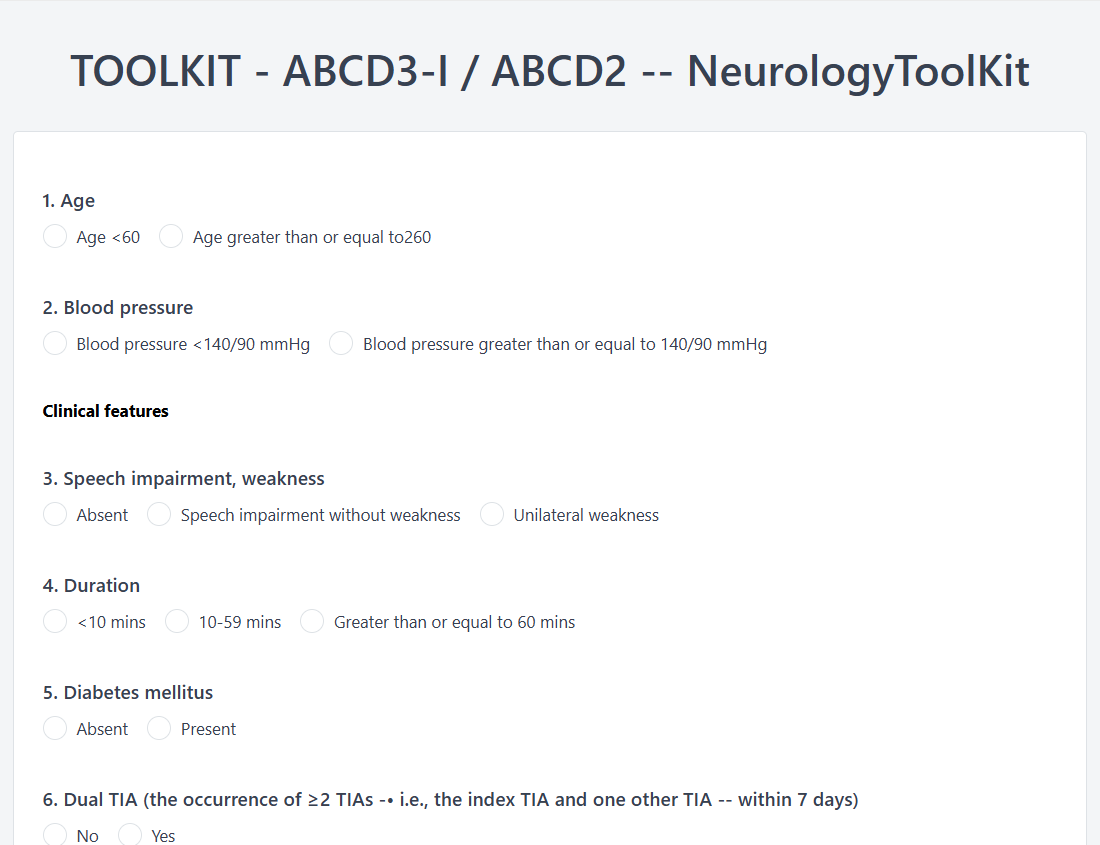
The ABCD3-I score adds up to 6 additional points to the ABCD2 for a maximum of 13:
ABCD3-I risk categories are: low risk (0–3), intermediate risk (4–7), and high risk (8–13). High-risk patients have an approximately 18% or greater 90-day stroke recurrence rate (Merwick et al., Lancet Neurology, 2010). Zentake automatically calculates both scores upon form submission, eliminating manual addition errors and enabling immediate risk stratification.
Step 1: Gather Clinical Parameters. Collect the patient's age, blood pressure reading, and diabetes status from their medical record or intake form. Zentake can pre-populate these fields from prior patient data.
Step 2: Assess Clinical Features. Document the patient's TIA symptoms — specifically whether unilateral weakness or isolated speech disturbance was present. Zentake's digital form uses dropdown selections to ensure consistent documentation.
Step 3: Record Symptom Duration. Determine how long TIA symptoms persisted. Zentake's form captures this in predefined time ranges to reduce ambiguity.
Step 4: Add Imaging Data (ABCD3-I only). If MRI DWI and carotid imaging are available, enter whether acute DWI abnormalities or ipsilateral carotid stenosis ≥50% were identified. Zentake's conditional logic shows these fields only when the ABCD3-I version is selected.
Step 5: Review Auto-Calculated Score. Zentake instantly computes the ABCD2 and/or ABCD3-I score, displays the risk category, and generates a summary for the patient's chart. Results can be sent directly to your EMR.
Scoring: Paper forms require manual point calculation, which is error-prone under time pressure. Zentake auto-calculates both ABCD2 and ABCD3-I scores instantly.
Completion: Paper forms take 3–5 minutes with manual math. Zentake's digital version completes in under 2 minutes with auto-populated fields.
Delivery: Paper forms must be physically handed to the clinician. Zentake forms can be completed on any device at the point of care.
Data Storage: Paper forms are filed in physical charts and difficult to retrieve. Zentake stores all submissions in encrypted, HIPAA-compliant cloud storage.
Longitudinal Tracking: Comparing paper scores across visits requires manual chart review. Zentake displays score trends over time in a dashboard.
Security: Paper forms risk loss, damage, or unauthorized access. Zentake uses end-to-end encryption and role-based access controls.
Integration: Paper scores must be manually transcribed into the EMR. Zentake integrates directly with systems like Elation, sending scores automatically.
Cost: Paper forms require printing and storage. Zentake eliminates these costs with unlimited digital submissions.
What does the ABCD2 score measure?
The ABCD2 score measures the short-term risk of stroke following a transient ischemic attack (TIA). It uses five clinical parameters — age, blood pressure, clinical features, symptom duration, and diabetes — to produce a risk score from 0 to 7. Higher scores indicate greater stroke risk within 2, 7, and 90 days. Zentake's digital version auto-calculates this score for faster clinical decision-making.
What is the difference between ABCD2 and ABCD3-I?
The ABCD3-I extends the ABCD2 by adding three imaging and clinical variables: dual TIA events within 7 days, ipsilateral carotid stenosis ≥50%, and acute DWI abnormality on MRI. This increases the score range from 0–7 to 0–13 and improves sensitivity from approximately 80% to 96% at 7 days (Merwick et al., 2010). Zentake supports both scoring systems in a single configurable form.
How do you score the ABCD2?
Sum points for: Age ≥60 (1 point), Blood Pressure ≥140/90 (1 point), Clinical features of unilateral weakness (2 points) or speech disturbance (1 point), Duration ≥60 min (2 points) or 10–59 min (1 point), and Diabetes (1 point). Scores of 0–3 are low risk, 4–5 moderate risk, and 6–7 high risk. Zentake handles all calculations automatically.
How long does it take to complete?
The ABCD2 takes approximately 1–2 minutes when clinical data is readily available. The ABCD3-I requires additional imaging results (DWI MRI and carotid imaging), which extends total assessment time depending on imaging availability. Zentake's digital form can be completed in under 2 minutes once all data is gathered.
Is the ABCD2 score free to use?
Yes, the ABCD2 and ABCD3-I scoring systems are freely available for clinical use. The scores are published in peer-reviewed literature and are not proprietary. Zentake provides a ready-to-use digital version that you can deploy immediately with a free trial.
Who should administer the ABCD2 or ABCD3-I?
These tools are designed to be administered by physicians, nurse practitioners, and physician assistants — particularly those in emergency medicine, neurology, and primary care settings. Any clinician evaluating a patient after a suspected TIA can use these scores. Zentake makes the tool accessible to all clinical team members with role-based permissions.
What population is the ABCD2 validated for?
The ABCD2 was validated in adult populations presenting with TIA. The original derivation and validation cohorts included over 4,800 patients across multiple international centers (Johnston et al., 2007). It is used in adults of all ages, though age ≥60 is one of the scoring parameters. Zentake's digital form can be used for any adult patient presenting with TIA symptoms.
Can the ABCD2 score be used alone to determine disposition?
Clinical guidelines recommend that the ABCD2 score be used as one factor in a comprehensive TIA evaluation, not as the sole determinant of patient disposition. A 2015 review noted that a substantial proportion of strokes (25%) occurred in patients with low or intermediate ABCD2 scores. Clinical judgment, imaging, and other factors should always be considered alongside the score.
1. Johnston SC, Rothwell PM, Nguyen-Huynh MN, et al. Validation and refinement of scores to predict very early stroke risk after transient ischaemic attack. Lancet. 2007;369(9558):283-292.
2. Merwick A, Albers GW, Amarenco P, et al. Addition of brain and carotid imaging to the ABCD2 score to identify patients at early risk of stroke after transient ischaemic attack: a multicentre observational study. Lancet Neurology. 2010;9(11):1060-1069.
3. Song B, Fang H, Zhao L, et al. Validation of the ABCD3-I score to predict stroke risk after transient ischemic attack. Stroke. 2013;44(5):1244-1248.
4. Wardlaw JM, Brazzelli M, Chappell FM, et al. ABCD2 score and secondary stroke prevention: meta-analysis and effect per 1,000 patients triaged. Neurology. 2015;85(4):373-380.
Last updated: March 2026
The leading patient intake platform. HIPAA compliant forms for healthcare providers and organizations. Find out what you're missing!



