

The Adult Brief Dissociative Experiences Scale–Modified (DES-B) is an 8-item self-report instrument that measures the frequency and severity of dissociative experiences — including depersonalization, derealization, amnesia, and identity confusion — in adults aged 18 and older. The DES-B was derived from the original 28-item Dissociative Experiences Scale (DES) developed by Bernstein and Putnam (1986) and refined by Dalenberg and Carlson (2010). Each of the 8 items is rated on a 5-point scale (0 = Not at all to 4 = More than once a day), yielding a total score of 0–32 and an average severity score of 0–4. A score of ≥30 on the raw total is considered clinically significant and warrants further evaluation. Internal consistency is high (Cronbach’s α > 0.90). Zentake delivers the DES-B as a HIPAA-compliant digital form with automated scoring and longitudinal tracking.
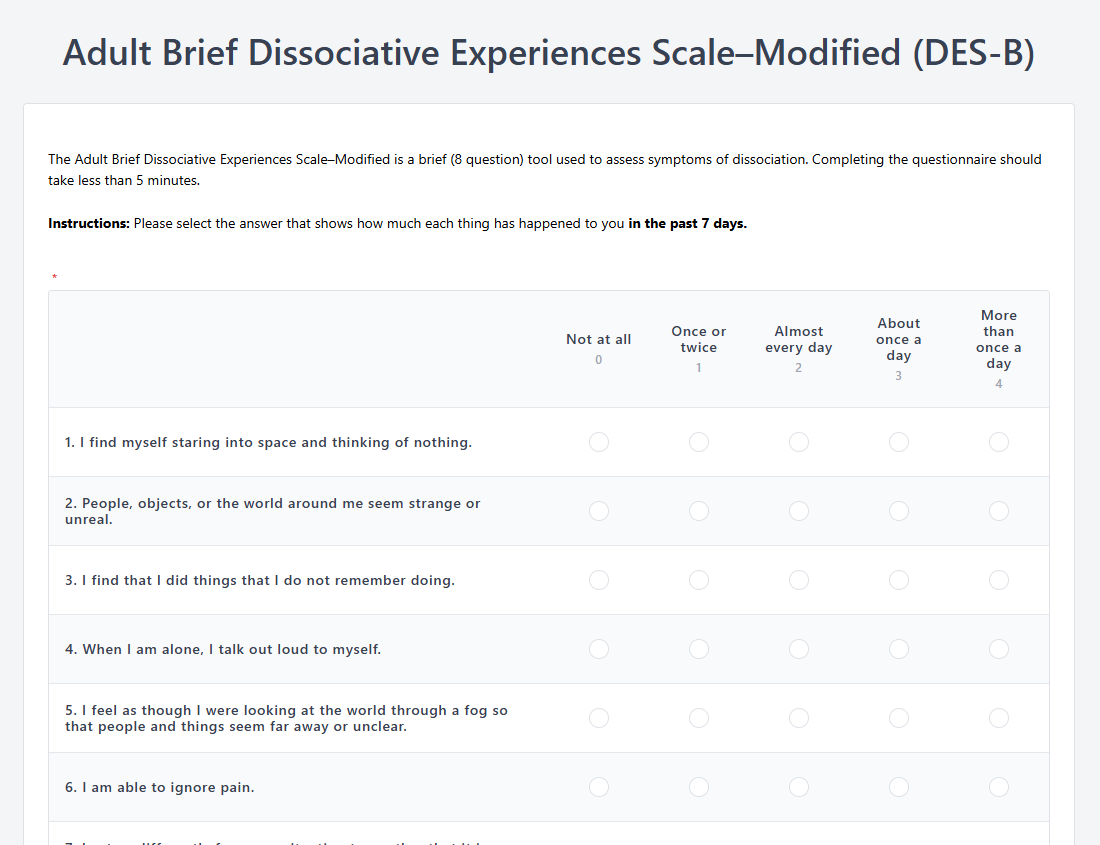
Each of the 8 items is rated on a 5-point frequency scale: 0 = Not at all, 1 = Once or twice, 2 = Almost every day, 3 = About once a day, 4 = More than once a day. The ratings reflect experiences over the past 7 days.
Total raw score: Sum all 8 items. Range: 0–32. Higher scores indicate greater dissociative severity.
Average severity score: Divide the total raw score by 8, yielding a 0–4 scale interpreted as: 0 = None, 1 = Mild, 2 = Moderate, 3 = Severe, 4 = Extreme.
Clinical cutoff: A raw total score of ≥30 indicates clinically significant dissociation and should prompt comprehensive diagnostic evaluation for dissociative disorders (Dalenberg & Carlson, 2010).
Missing data rule: If 3 or more items are unanswered, the total score should not be calculated. If 1–2 items are missing, prorate: sum answered items × 8 ÷ number of items answered.
Zentake automatically calculates both the raw total and average severity score upon submission, applying the prorating rule when applicable, and flags scores at or above the clinical cutoff for immediate clinician attention.
Step 1: Confirm the appropriate population. The DES-B is validated for adults aged 18 and older. It is most commonly used in trauma-informed care settings, PTSD evaluations, and dissociative disorder assessments. Zentake’s intake workflow lets you configure the DES-B to route automatically to appropriate patient populations based on your clinical criteria.
Step 2: Deliver before the clinical session. Send the DES-B via Zentake’s secure patient portal or text/email link prior to the appointment. Asking patients to reflect on dissociative experiences in a comfortable, private setting — rather than a waiting room — typically yields more accurate self-report.
Step 3: Provide clear instructions. Instruct the patient to rate how often each experience has happened to them in the past 7 days, selecting the frequency that best applies. Zentake’s digital form presents instructions inline so patients can reference them as needed.
Step 4: Review scores automatically. Zentake calculates the raw total and average severity score the moment the patient submits, delivering the scored result to the clinician’s dashboard before the session begins. Scores at or above the clinical cutoff are automatically flagged.
Step 5: Interpret in clinical context and follow up. A high DES-B score is not a diagnosis. Clinically elevated scores should prompt structured clinical assessment for dissociative disorders (using tools such as the SCID-D), trauma history review, and consideration of differential diagnoses including PTSD, borderline personality disorder, and substance-induced states. Zentake’s longitudinal tracking allows re-administration at follow-up visits to monitor symptom change across treatment.
Scoring: Paper requires manual summation of 8 items and manual application of the prorating rule for missing data — prone to calculation errors. Zentake applies the exact scoring algorithm automatically, including prorating.
Completion: Paper forms handed out during the clinical encounter interrupt the rapport-building of the session. Zentake sends the DES-B before the appointment so patients arrive pre-screened.
Delivery: Paper is limited to in-person distribution. Zentake supports text, email, and portal delivery for telehealth and multi-site practices.
Data Storage: Paper DES-B forms require secure filing and manual transcription. Zentake stores all responses in encrypted, HIPAA-compliant cloud storage with instant search and retrieval.
Longitudinal Tracking: Monitoring dissociative symptom change across treatment requires comparing multiple paper forms manually. Zentake’s Measures dashboard graphs DES-B scores across visits automatically.
Security: Paper forms can be lost, misfiled, or accessed without authorization — a significant risk for sensitive trauma-related disclosures. Zentake provides role-based access controls and complete audit logging.
Integration: Paper scores must be manually entered into the EHR. Zentake integrates with leading EMR systems to push results directly to the patient chart.
Cost: Paper incurs printing, storage, and labor costs. Zentake replaces all of these with a scalable digital workflow.
What does the DES-B measure?
The DES-B measures the frequency and severity of 8 core dissociative experiences over the past 7 days — including depersonalization (feeling detached from one’s body or thoughts), derealization (feeling that the environment is unreal), dissociative amnesia (gaps in memory), and absorption (becoming so engrossed in something that awareness of surroundings is lost). It was designed to efficiently capture the full range of pathological dissociation covered in the original 28-item DES. Zentake’s digital version delivers these 8 items with auto-scoring and immediate results.
How do you score the DES-B?
Sum all 8 item ratings (each 0–4) for a total raw score of 0–32. Divide by 8 for the average severity score (0–4). A raw total of ≥30 is clinically significant. If 1–2 items are missing, prorate: (sum of answered items × 8) ÷ number answered. If 3+ items are missing, do not score. Zentake applies all of these rules automatically.
How long does the DES-B take to complete?
The DES-B typically takes 2–5 minutes to complete. Its 8-item brevity makes it practical for routine clinical intake without adding significant burden to patients, even those in acute distress.
Is the DES-B free to use?
The DES-B is available for clinical and research use. Zentake provides a pre-built digital version with automated scoring as part of its template library. Start a free trial to access the DES-B and hundreds of other validated clinical assessments.
What age or population is the DES-B validated for?
The DES-B is validated for adults aged 18 and older. It has demonstrated high measurement invariance across ethnoracial groups (Dalenberg et al., 2023), supporting its use in diverse clinical and community samples.
Who should administer the DES-B?
The DES-B is a self-report screener that patients complete independently. It is most appropriately deployed by licensed mental health clinicians — psychologists, psychiatrists, licensed clinical social workers, or trauma therapists — as part of a broader trauma or dissociative disorder assessment. Results should always be interpreted in clinical context, not used to diagnose dissociative disorders without a comprehensive evaluation.
What is the difference between the DES-B and the full DES?
The original DES (Bernstein & Putnam, 1986) contains 28 items rated on a 0–100% visual analog scale. The DES-B is an 8-item abbreviated version using a simpler 0–4 frequency scale, retaining the core dissociative content while reducing respondent burden. Psychometric properties of the DES-B are comparable to the full scale (Cronbach’s α > 0.90), making it well-suited for routine clinical screening.
Can the DES-B diagnose dissociative identity disorder (DID)?
No. The DES-B is a symptom severity screener, not a diagnostic instrument for DID or other specific dissociative disorders. Elevated scores indicate the need for comprehensive clinical evaluation, including structured diagnostic interviews such as the SCID-D. A diagnosis of DID or any dissociative disorder must be made by a qualified clinician following DSM-5 or ICD-11 criteria.
1. Bernstein EM, Putnam FW. Development, reliability, and validity of a dissociation scale. Journal of Nervous and Mental Disease. 1986;174(12):727–735.
2. Dalenberg CJ, Carlson EB. Dissociation in posttraumatic stress disorder part II: how theoretical models fit the empirical evidence and recommendations for modifying the diagnostic criteria for PTSD. Psychological Trauma: Theory, Research, Practice, and Policy. 2012;4(6):551–559.
3. Dalenberg CJ, Briere J, Sedler M, et al. Development of a Brief Version of the Dissociative Symptoms Scale and the Reliability and Validity of DSS-B Scores in Diverse Clinical and Community Samples. Assessment. 2023. PMC10478338.
Last updated: March 2026
The leading patient intake platform. HIPAA compliant forms for healthcare providers and organizations. Find out what you're missing!



